The American Society for Clinical Pathology’s 2017 Wage Survey of Medical Laboratories in the United States: Executive Summary
By - June 29, 2022

Since 1988, the American Society for Clinical Pathology (ASCP) has conducted its biennial Wage Survey to inform the pathology and laboratory field of the most recent national wage data. The 2017 Wage Survey was conducted through collaboration between the ASCP’s Institute of Science, Technology, and Policy in Washington, D.C., and its Board of Certification in Chicago. The Wage Survey Working Group, whose members work in the field of pathology and laboratory medicine, reviewed the survey questions and critiqued the report. Partner organizations were also invited to participate.
The survey was conducted between April 3 and May 3, 2018, via Key Survey, an online survey tool. Participants were recruited through broadcast emails. Snowball sampling method was used to maximize survey participation. Eligible participants included laboratory professionals currently employed in a medical laboratory in the U.S. or U.S. territories. However, information was also collected from those disqualified from the wage survey for future research.
A total of 14,628 responses were received in the 2017 wage survey. Demographic data collected indicate that majority of the respondents were females (80.50%) and identified as White or Caucasian (74.10%), with an average age of 42.89 years (compared to 43.95 years in 2015 wage survey). Most common occupational titles described by the participants were medical laboratory scientist/medical technologist/clinical laboratory scientist (50.05%), followed by medical laboratory technician/clinical laboratory technician (16.04%), phlebotomist (7.45%), histotechnician (4.89%), and cytotechnologist (2.83%). Occupational levels included staff (63.62%), lead (11.99%), supervisor (12.01%), manager (6.03%), director (3.35%), and other (3.05%). The top 10 states providing most survey responses were: Texas (7.80%), California (5.90%), New York (4.80%), Illinois (4.40%), Ohio (4.20%), Wisconsin (3.90%), Pennsylvania (3.80%), Florida (3.80%), Minnesota (3.70%), Michigan (3.40%), and North Carolina (3.30%). By region, the respondents are from South Central Atlantic (23.87%), Far West (18.87%), Central North East (19.12%), Northeast (15.71%), Central South West (11.25%), and Central North West (11.18%). Survey respondents are mostly from urban areas (66.62%,) followed by urban clusters (6.86%) and rural areas (6.52%).
Most participants held full-time positions (89.23%) and were trained from a National Accrediting Agency for Clinical Laboratory Sciences accredited or approved training program (49.47%). Majority were employed in academic and nonacademic hospital facilities and worked in the hematology/coagulation department. Participants had a high certification rate (91.64%), with most certified by ASCP Board of Registry/Certification or National Certification Agency (86.10%). Overall, 29.45% are licensed by the state of current employment, with most working in California. In total, 7.5% of respondents reported being represented by a union, most commonly by SEIU 1199 (28.50%). Individuals excluded from the survey were those who are unemployed (17.68%), working in a laboratory-related industry (14.29%), retired (11.70%), a clinical laboratory educator (8.30%), working in a research laboratory (eg, biotech industries) (4.11%), and other (32.4%).
Overall, phlebotomists (PBT) and clinical laboratory assistant/medical laboratory assistants (CLA/MLA) reported lower salaries, while pathologists’ assistants (PA) and performance improvement or quality assurance personnel reported higher salaries than the rest of the laboratory professions (Table 1). Breakdown of these salaries by occupational levels produces similar results, with highest staff-level salaries for PAs and lowest for PBTs (Figure 1). Compared to 2015 ASCP wage survey, results from this survey show an increase in wages for most laboratory occupations. Analysis by geographic area type revealed higher hourly wages for laboratory professionals working in urban areas, compared to overall estimates for most occupational titles (Table 1).
Table 1. Average hourly wage by occupational title and geographical areas.
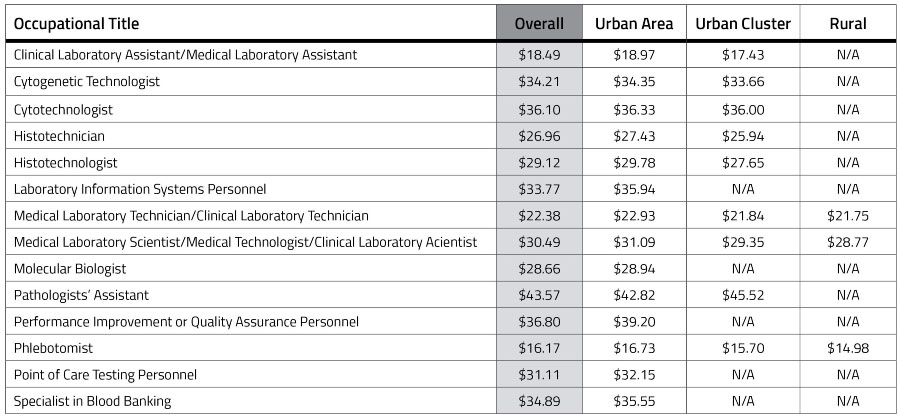
Sample size constraints prevented further analysis of wage rate for some occupational levels. Urban area, 50,000 people or more; Urban cluster, between 2,500 and 50,000 people; Rural, 2,500 people or less.
Figure 1. Average hourly wage for laboratory staff, lead, supervisor/manager, and director positions, per occupational title.

Sample sizes for some occupational levels were less than 30 (n<30) and did not allow for statistically significant comparisons. CLA/MLA, clinical laboratory assistant/medical laboratory assistant; CG indicates cytogenetic technologist; CT, cytotechnologist; HT, histotechnician; HTL, histotechnologist; LIS, Laboratory Information Systems Personnel; MLT/CLT, medical laboratory technician/clinical laboratory technician; MLS/MT/CLS, medical laboratory scientist/medical technologist/clinical laboratory scientist; MB, molecular biologist; PA, pathologists’ assistant; PI or QA, performance improvement or quality assurance ; PBT, phlebotomist; POCT, point of care testing personnel; SBB, specialist in blood banking.
Compared to wage results of 2015, the increase in wages of laboratory professionals as they accumulate more years of experience in the field is higher in the 2017 wage survey. The 2017 survey shows a slightly younger demography compared to last time, except for CGs and CTs. Younger workforce is perhaps the result of high retirement rates occurring in the field.2 In general, the salaries were higher with increasing age groups across the occupational titles. Analysis of wage by gender showed that for most occupational titles, males earned more than females with PAs reporting the greatest difference in salaries. Survey respondents were asked about the benefits and perks they receive from their institution, and medical/dental/vision, pension/retirement, overtime/holiday/weekends, and employee parking continue to be the top fringe benefits they receive.
The primary themes revealed from the qualitative analysis of the 1,452 comments from the survey participants were appreciation for the survey (42.91%), being underpaid (with low yearly increase and low maximum pay)/underappreciated (especially compared to nursing and other allied health professions) (39.39%), suggestions for future surveys (9.02%), request for more data on wages by region/location, with participants from rural areas commenting on low wages and lack of staff leading to early burnout and those belonging to urban areas noting wages not being enough to meet the high cost of living (4.48%), lack of appreciation and recognition from their peers (2.96%), certification related (2.82%), benefits related (2.41%), union membership (2.27%), education and training (2.07%), hiring and retention (1.86%), concerns over retirements (0.96%), licensure (0.62%), and concerns over nursing personnel performing laboratory tests (0.55%). As noted in the previous survey, institutions are encouraged to consider the level of education, training, years of experience, cost of living and pay structure of other allied health professionals when deciding the laboratory professionals’ compensation. The U.S. Bureau of Labor Statistics (BLS) reported that the job outlook for medical and clinical laboratory technologists and technicians between 2016 and 2026 is expected to grow 13%, which is faster than the average rate.2 The BLS also indicated that an increase in the aging population is expected to lead to a greater need to diagnose medical conditions, such as cancer or type 2 diabetes, through laboratory procedures.2 Data from the 2016 Vacancy Survey strongly suggest the crucial need in the supply of qualified and certified laboratory personnel, highlighting the need for strategic focus on recruitment.3
For supervisors in rural areas and small community hospitals, vacancies have been open for many months, leaving their laboratories with heavier workloads. As retirement rates continue to increase, the field needs to intensify its efforts on recruiting the next generation of laboratory personnel. This can be accomplished by enrolling more students in accredited training programs and helping them gain necessary experience to become certified. Retention of new graduates is critical, and the staffing needs of rural areas need to be highlighted.3 According to James Wisecarver, MD, PhD, FASCP, strengthening the workforce can also be met through education and awareness of the excellent career opportunities available to individuals in this field.4 He also encourages the field to be actively engaged with the policy makers at both the federal and state levels if we are to be successful in raising awareness about the value of the profession and the anticipated workforce shortages. The full 2017 ASCP Wage Survey Report is available at academic.oup.com/ajcp.
References
- US Bureau of Labor Statistics. CPI inflation calculator. https://www.bls.gov/data/inflation_calculator.htm
Accessed June 2, 2018. - US Bureau of Labor Statistics. Occupational Outlook Handbook. www.bls.gov/ooh/healthcare/medical-and-clinical-laboratory-technologists-and-technicians.htm.
Accessed June 3, 2018. - American Society for Clinical Pathology. The American Society for Clinical Pathology’s 2016–2017 Vacancy Survey of medical laboratories in the United States. doi.org/10.1093/ajcp/aqy005.
Accessed June 4, 2018. - Wisecarver JL. Strengthening the workforce through education. Critical Values. 2018;11:6-8.

Edna Garcia and Iman Kundu
ASCP research and analytics